A BMD test is
the only way to detect low bone density and diagnose osteoporosis. The
lower a person’s bone mineral density, the greater the risk of having a
fracture. A BMD test is used to:
- Detect low bone density before a
person breaks a bone
- Predict a person’s chances of breaking
a bone in the future
- Confirm a diagnosis of osteoporosis
when a person has already broken a bone
- Determine whether a person’s bone
density is increasing, decreasing or remaining stable (the same)
- Monitor a person’s response to
treatment
Who Should Have a BMD Test?
There are some reasons (called risk factors) that increase your
likelihood of developing osteoporosis. The more risk factors you have,
the more likely you are to get osteoporosis and broken bones. Some
examples are being small and thin, older age, being female, a diet low
in calcium, lack of enough vitamin D, smoking and drinking too much
alcohol.
Your healthcare provider may recommend a
BMD test if you are:
- A postmenopausal woman under age 65
with one or more risk factors for osteoporosis
- A man age 50-70 with one or more risk
factors for osteoporosis
- A woman age 65 or older, even without
any risk factors
- A man age 70 or older, even without
any risk factors
- A woman or man after age 50 who has
broken a bone
- A woman going through menopause with
certain risk factors
- A postmenopausal woman who has stopped
taking estrogen therapy (ET) or hormone therapy (HT)
Some other reasons your healthcare
provider may recommend a BMD test:
- Long-term use of certain medications
including steroids (for example, prednisone and cortisone), some
anti-seizure medications, Depo-Provera®
and aromatase inhibitors (for example, anastrozole, brand name
Arimidex®)
- A man receiving certain treatments for
prostate cancer
- A woman receiving certain treatments
for breast cancer
- Overactive thyroid gland
(hyperthyroidism) or taking high doses of thyroid hormone medication
- Overactive parathyroid gland
(hyperparathyroidism)
- X-ray of the spine showing a fracture
or bone loss
- Back pain with a possible fracture
- Significant loss of height
- Loss of sex hormones at an early age,
including early menopause
- Having a disease or condition that can
cause bone loss (such as rheumatoid arthritis or anorexia nervosa)
Types of Bone Density
Tests
Central DXA: The National Osteoporosis Foundation (NOF)
recommends a BMD test of the hip and spine by a central DXA machine to
diagnose osteoporosis. DXA stands for dual energy x-ray absorptiometry.
When testing can’t be done on the hip and spine, NOF suggests a central
DXA test of the radius bone in the forearm. In some cases, the type of
bone density testing equipment used depends on what is available in your
community.
Healthcare providers measure BMD in the hip and spine for several
reasons. First, people with osteoporosis have a greater chance of
fracturing these bones. Second, these fractures can cause more serious
problems, including longer recovery time, greater pain and even
disability. BMD test results in the hip and spine can predict the
likelihood of future fractures in other bones.
With most types of BMD tests, a person remains fully dressed, and the
test usually takes less than 15 minutes. BMD tests are non-invasive,
meaning that no needles or instruments are placed through the skin or
body. When repeating a BMD test, it is best to use the same testing
equipment and have it done at the same place. This provides a more
accurate comparison with your last test result.
Although it is not always possible to have your BMD test at the same
place, it is still important to compare your current BMD test to your
last one.
Other Types of Tests:
In addition to central DXA, there are other methods to measure bone
density that can predict the risk of breaking a bone. However, the
results from these other methods are not equivalent to the results from
a central DXA machine. Below are other BMD testing methods:
- pDXA (peripheral dual energy x-ray
absorptiometry)
- QUS (quantitative ultrasound)
- QCT (quantitative computed tomography)
- pQCT (peripheral quantitative computed
tomography)
The QUS method of BMD testing uses sound
waves to measure bone density. The other types of equipment listed above
use radiation. Except for QCT, the amount of radiation is very small.
For comparison, you are exposed to 10–15 times more radiation flying in
a plane round trip between New York and San Francisco.
Healthcare providers do not routinely use standard x-rays for BMD
testing. While x-rays can identify broken bones, they are not sensi-tive
enough to detect osteoporosis until 25 to 40 percent of bone density has
been lost. By this time the disease is well advanced.
Screening Tests
Peripheral bone mineral density tests help identify people who are most
likely to benefit from further BMD testing. This type of test is often
done as a screening at health fairs and in some medical offices, but
cannot be used to accurately diagnose osteoporosis. Peripheral BMD tests
measure BMD in the extremities, including the forearm, wrist, finger or
heel. This BMD testing method uses pDXA, QUS and pQCT.
People having a peripheral test should be aware that there are some
limitations with this type of test. Comparisons between a peripheral
test and a DXA test of the hip and/or spine may not be reliable.
Peripheral tests are suitable for screening and
predicting the risk of fractures. Experts prefer the central DXA test
for diagnosing osteoporosis and monitoring treatment in patients taking
an osteoporosis medication.
If you have abnormal results from a peripheral BMD screening, you should
follow up with your healthcare provider. Discuss whether you need
additional testing, such as a central DXA test of the hip and/or spine.
People of Larger Size
Most central DXA machines cannot measure BMD in the hip and spine of
patients who weigh over 300 pounds. Some newer machines can measure BMD
in people who weigh up to 400 pounds, but they are not widely available.
When the hip and spine cannot be measured, a central DXA test can often
measure BMD of the radius bone in the forearm to diagnose osteoporosis.
If this can’t be done, another option is a peripheral BMD test of
another extremity, such as the heel or wrist.
For people of larger size, some healthcare providers recommend having
both a central DXA test of the forearm and a peripheral test of the heel
or other bone. Doing both of these tests provides more complete
information.
How Often to Repeat a BMD
Test
People taking an osteoporosis medication should repeat their BMD test by
central DXA every two years, according to the National Osteoporosis
Foundation (NOF). Some healthcare providers may have certain patients
repeat their BMD test after one year. The peripheral tests (pDXA, QUS
and pQCT) are not appropriate for monitoring response to treatment at
this time.
Tests to Find Broken Bones
If you have a loss of height, posture changes or back pain, your
healthcare provider may order an x-ray to look for fractures in your
spine. An x-ray is the most common way to tell if you have a broken bone
in your spine or other bones. In some people, spine fractures don’t
cause any pain.
Once you have a fracture in the spine, you are at greater risk for more
spine fractures in the future. If you have this type of fracture, that’s
why you need to speak with your healthcare provider about steps to
protect your spine. You should also consider treatment with an
osteoporosis medication. When you have a fracture in the spine, you
still need to have a BMD test if you haven’t had one.
Another way to find fractures in the spine is with a vertebral fracture
assessment (VFA) by a DXA machine. This method uses less radiation than
a standard x-ray. VFAs can show breaks in the spine and can also show
the difference between broken bones and abnormally shaped bones.
Understanding BMD Test Results
When you have a bone mineral density test, it compares your bone density
to a “young normal” healthy 30-year-old adult with peak bone density
(also called peak bone mass). Peak bone density is the point at which a
person has the greatest amount of bone that she or he will ever have.
You will get the result of your BMD test in a special number called a
T-score. It stands for “standard deviations” or “SD.” It indicates how
much your bone density is above or below normal.
Healthcare providers use the T-score to diagnose osteoporosis. If
more than one bone is tested, they use the lowest T-score to make a
diagnosis of osteoporosis. The World Health Organization (WHO) has
defined the T-scores and what they mean.
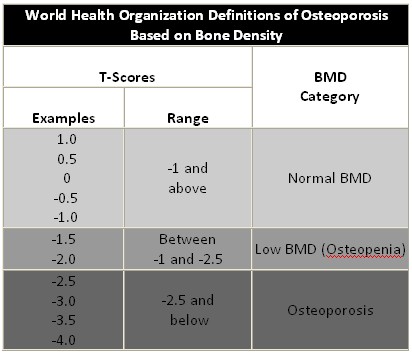
What your T-score means:
- A T-score between +1 and -1 is normal
bone density. Examples are 0.8, 0.2 and -0.5.
- A T-score between -1 and -2.5
indicates low bone density or osteopenia. Examples are T-scores of
-1.2, -1.6 and -2.1.
- A T-score of -2.5 or lower is a
diagnosis of osteoporosis. Examples are T-scores of -2.8, -3.3 and
-3.9.
The lower a person’s T-score, the lower
the bone density. A T-score of -1.0 is lower than a T-score of 0.5; a
T-score of -2.0 is lower than a T-score of -1.5; and a T-score of -3.5
is lower than a T-score of -3.0.
For most BMD tests, 1 SD difference in a T-score equals a 10-15 percent
decrease in bone density. For example, a person with a T-score of -2.5
has a 10-15 percent lower BMD than a person with a T-score of -1.5.
Your BMD test result also includes a Z-score that compares your
bone density to what is normal in someone your age and body size.
Healthcare providers do not use Z-scores to diagnose osteoporosis in
postmenopausal women and men age 50 or older. Among older adults low
bone mineral density is common, so Z-scores can be misleading. An older
person might have a “normal” Z-score but still be at high risk for
breaking a bone.
Most experts recommend using Z-scores rather than T-scores for younger
men, premenopausal women and children. However, healthcare providers
often use
T-scores for perimenopausal women. A Z-score above -2.0 is normal
according to the International Society for Clinical Densitometry (ISCD).
A diagnosis of osteoporosis in younger men, premenopausal women and
children should not be based on a BMD test result alone. NOF does not
recommend routine BMD testing in children, adolescents, healthy young
men or premenopausal women.
When to Consider Treatment
The results of the BMD test help your healthcare provider make
recommendations about either prevention or treatment of osteoporosis.
When making a decision about treatment with an osteoporosis medication,
your healthcare provider will also consider your risk factors for
osteoporosis, your likelihood of having future fractures, your medical
history and your current health.
Below are treatment guidelines for postmenopausal women and men age 50
or older:
- Most people with T-scores of -1 and
above (normal bone density) do not need to take an osteoporosis
medication.
- People with T-scores between -1 and
-2.5 (osteopenia) should consider taking an osteoporosis medication
when they have certain risk factors.
- All people with T-scores of -2.5 and
below (osteoporosis) should consider taking an osteoporosis
medication.
A new method called absolute fracture
risk helps healthcare providers and their
patients age 40 and older make better decisions about when to take an
osteoporosis medication. Absolute fracture risk estimates a person’s
chance of breaking a bone over a period of 10 years. Postmenopausal
women and older men with osteoporosis are at greatest risk of breaking a
bone.
In the past, healthcare providers knew to treat people with
osteoporosis, but were sometimes uncertain about when to treat patients
with osteopenia. The absolute fracture risk method makes it easier for
healthcare providers and their patients with osteopenia to decide when
an osteoporosis medication is necessary. This method helps make sure
that people with the greatest chance of breaking a bone get treated.
Healthcare providers can get a patient’s absolute fracture risk by using
a special web-based tool on a computer in their office. The healthcare
provider enters a patient’s hip T-score and certain risk factors for
osteoporosis. The tool predicts the patient’s absolute fracture risk.
Soon, some central DXA machines will be able to provide this
information.
Osteoporosis medications
either slow or stop bone loss or
rebuild bone. They also reduce the chances of having a broken bone. NOF
encourages you to discuss your treatment options with your healthcare
provider. Always look at both the risks and benefits of taking a
medication, including potential side effects.
For an osteoporosis medication to work, a person still needs to get
enough calcium and vitamin D and to exercise. According to NOF
recommendations, adults under age 50 need 1,000 mg of calcium and
400-800 IU of vitamin D daily. Adults 50 and over need 1,200 mg of
calcium and 800-1,000 IU of vitamin D daily. There are two types of
vitamin D supplements. They are vitamin D3 and vitamin D2. Previous
research suggested that vitamin D3 was a better choice than vitamin D2.
However, more recent studies show that vitamin D3 and vitamin D2 are
equally good for bone health. Vitamin D3 is also called cholecalciferol.
Vitamin D2 is also called ergocalciferol.
Note: This information is from the National Osteoporosis
Foundation website. Visit the NOF website at
www.nof.org for further information.
Back to Innovative Technologies
|
Top of Page |
Home Page |